HANOVER, IN (WAVE) – A Madison, Ind., man is behind bars, accused of raping a dementia patient.
David
Garcia is charged with one count of rape, a level-three felony. Hanover
police said it happened Saturday at the Hanover Nursing Center. Garcia
was arrested Wednesday after a co-worker reported him having sex with a
74-year-old female dementia patient.
“He
had been a past employee there and had returned recently to it as a CNA
or certified nursing assistant,” said Chief Joshua Taylor, of the
Hanover Police Department. “That’s the position he was working in the
capacity of this evening.”
According
to police records, a co-worker saw a man with his pants down and a
woman on the bed, believed to be a patient, and reported it to
co-workers immediately to be investigated.
When questioned, the victim told investigators she’d had sex with a man and pointed toward her groin.
“As
of right now, with the information we have, we felt comfortable filing
that rape charge, but will continue to review this going forward, if any
additional charges will pop up during the investigation,” Jefferson
County (Ind.) Prosecutor David Sutter said.
Garcia
admitted he was in that room but denied the alleged assault, trying to
explain to police why his bodily fluids may have been in the room.
Police
said Garcia had prior arrests but nothing like this. Taylor said it’s
so important to be careful when hiring people in charge of caring for
vulnerable populations, like dementia patients.
“You
do everything you can to ensure you have the right person for the
position there,” Taylor said. “From the get go, a lot of times with
investigations we have, there’s no indicators, nothing in the history,
nothing in past to give the red flag.”
If convicted, Garcia could face up to 16 years in prison.
Sutter
said his office is weighing the charges in the case seriously because
of the kind of crime and the position of trust Garcia was in during the
alleged rape.
“As
a community, you always want to try to take care of your most
vulnerable,” Sutter said. “We certainly feel like whether it’s infants
or folks that are for whatever reason in nursing centers, those are
people that we need to take care of and we obviously take that very
seriously. Community safety is the utmost importance for my office and
the Hanover Police Department.”
Hanover
police said the investigation is ongoing, and they’re speaking with
others at the nursing center to ensure there are no other victims but
right now, they believe this was an isolated incident.
Garcia is expected to be in court Friday for an initial hearing.
The administrator at the Hanover Nursing Center declined to comment
about the incident or about Garcia’s arrest, saying she couldn’t discuss
the matter while it’s under investigation.
Maine Board of Overseers of the Bar announced Wednesday that
Brunswick lawyer James Whittemore will not be allowed to practice law
for 10 years, citing serious professional and ethical violations that
include allegations he has misused approximately $287,000 of client
funds.
The Times Record
reported by Whittemore, 69, also faces criminal charges in Cumberland
County. He was indicted on two counts of theft by misapplication of
property and one count of theft by unauthorized taking, the Brunswick
newspaper reported, adding that Whittemore pleaded not guilty to those
charges.
"In each instance, Mr. Whittemore's conduct demonstrated
violations of duties owed directly to his clients," Superior Court
Justice Nancy D. Mills wrote in her Nov. 30 decision. "In addition, Mr.
Whittemore violated duties that he owed to the court, to the public, and
to his profession. … As noted above, in each of the five counts, there
was serious and intentional misconduct that exacted both financial and
emotional injury to vulnerable clients."
Mishandled
and is suspected of converting "approximately $151,981.06 derived from
the assets" of a trust in "a matter then pending in the Cumberland
County Probate Court."
Improperly received and converted
$100,000 in a settlement of two wrongful death claims, which had been
made directly payable to his client trust account instead of the client
and her son.
Misappropriated $15,000 sent by a donor to the Brunswick-Topsham Land Trust to be held in escrow for an easement purchase.
Accepted
$18,790 from a client he was representing in a "right-of-way easement
issue … without performing the requisite legal work."
Accepted a
$1,500 retainer from a client and "performed minimal legal services for
[the client] and then converted the remaining advanced fee for his own
use."
Court documents indicate the complainants have filed
or will be filing for reimbursement through the Lawyer's Fund for Client
Protection.
The Times Record reported that Whittemore's lawyer declined comment on the case on Wednesday.
Like
many Americans, I have a story about hospice care for a loved one. When
my father was dying from complications of dementia and diabetes,
hospice caregivers sat with him, provided pain relief, and helped him be
comfortable. They also gave my mother peace of mind that her beloved
husband was receiving kind attention in his final weeks. To this day,
she refers to those hospice workers as angels.
Sadly, not every family’s story is a positive one.
Some patients experience days of pain or severe
anxiety because their hospices fail to provide pain management and other
needed services. Some are signed up for hospice without their
knowledge, including some individuals who are not terminally ill.
The Department of Health and Human Services’ Office of Inspector General, for which I work, recently published a report
examining hospice practices over a decade. It showed that hospices do
not always provide the services that patients need and sometimes provide
poor-quality care. We also found that patients and their families often
do not receive crucial information to make informed decisions about
hospice care.
We uncovered multiple abuses in our investigations:
Hospice recruiters inappropriately promised Medicare
beneficiaries free housecleaning and other services that are not
provided through hospice without telling them they would be signed up
for the hospice benefit. That means they unknowingly gave up treatments
that could cure, or at least manage, their conditions and instead
received only palliative care.
In a North Texas case, nurses allegedly gave high doses of drugs such
as morphine, regardless of whether patients needed it, to justify
receiving the higher hospice payments. Some of these excessive dosages
resulted in significant injury or death.
Or take the case of Larry Johnson’s 87-year-old mother, who had
dementia. Two days before she died, he learned that she had been
enrolled in hospice more than a year earlier, a decision that an
individual with dementia shouldn’t make without assistance. “My mother
needed basic care, but not hospice ― and especially not for a year and
then some!” Johnson said in an interview with our staff.
Our investigation in her case yielded results: The owner of that
hospice company received a 6-1/2-year federal prison sentence for
running an elaborate, $20 million hospice scheme that signed up patients
who were not dying. The hospice is permanently closed.
The idea that hospice care could abuse and neglect patients when they
are at their most vulnerable, or exploit them for unjust enrichment, is
repellent.
Because taxpayers bankroll poor care and fraud through the Medicare
hospice benefit, policymakers need to take immediate action to implement
safeguards against fraud, waste, and abuse of this important benefit.
Growth in the use of hospice makes it even more important to take
action now. The latest Medicare data show that hospice use has grown
over the past decade: In 2006, Medicare paid $9.2 billion for fewer than
1 million beneficiaries in hospice care. Ten years later, it paid $16.7 billion for more than 1.4 million beneficiaries.
Quality hospice care can provide significant comfort and support to
terminally ill patients and their families and caregivers. But we must
take steps to prevent both the very human toll and the economic toll
that hospice fraud takes.
The Inspector General’s office made recommendations to the Centers
for Medicare and Medicaid Services, which runs Medicare, in seven key
areas. Although CMS did not agree with a number of them, we believe they
are essential for weeding out poorly performing and unscrupulous
hospice providers:
Congress should give CMS the authority to hold poor performing hospices accountable and take swift action when warranted.
CMS should take steps to tie payments to patient care needs and
quality of care, rather than the current approach of paying a flat rate
regardless of how many services a hospice provides, which can create
incentives to minimize services and seek patients with uncomplicated
needs.
CMS should provide more information to the public, especially
Medicare beneficiaries, about hospice performance so consumers can
effectively compare hospice providers. CMS now provides such information
for nursing homes on its Nursing Home Compare website; a similar
offering for hospice on Hospice Compare would help consumers make
informed choices.
Patients and their family members can help guard against fraud by
carefully reviewing the summary notices they receive from Medicare
detailing the services for which Medicare has been billed on their
behalf and report those that were not authorized or received.
Medicare beneficiaries who elect hospice care should receive
high-quality services, and hospices should act with integrity when
billing government health programs. Most already do that, and assist
dying patients with dignity and compassion.
We strongly urge CMS and Congress to implement our longstanding
recommendations to protect patients and their families from hospice
providers that are exploiting this vital service.
Joanne M. Chiedi is the principal deputy inspector general for the Department of Health and Human Services.
It’s been more than a year since
81-year-old Toronto nursing home resident Phillip Kennedy suffered a leg
wound so deep and wide it looked as if he had been sliced open by an
axe.
His daughter, Kathleen Kennedy, said the home has never told
her family how Phillip was injured, even though it happened in the
middle of the day, in a licensed Ontario long-term care facility busy
with nurses and personal support workers.
Kathleen
Kennedy, with her brother Greg with their mother, Teresa. Phillip Kennedy went into a Toronto nursing home on Oct. 25 2017 for a short
rehab stay and three days later, suffered a massive gash that was so
deep it lookedlike someone had struck him with an axe. (Steve Russell / Toronto Star)
When
Phillip was injured — three days after moving in — nobody from
Hawthorne Place Care Centre could, or would, say how it happened. A
provincial ministry of health inspector spent six days investigating but
found no explanation for the cause of the injury. Phillip died in
hospital three weeks later. Kathleen said his death report cited
end-stage heart disease and kidney failure.
“If they had just said
to me, ‘you know what, we dropped him,’ or even, ‘you know what, he was
hit with an axe, we are sorry and this is what we’ve done to make sure
it doesn’t happen to someone else,’ I would have accepted it. But there
was none of that. Nothing,” Kathleen said.
“It is very unsettling.”
After
Phillip was injured, on Oct. 28, 2017, the inspector interviewed at
least eight employees, including the home’s administrator,
physiotherapist and personal support workers. While the inspector’s
final report, provided to the Star by Phillip’s family, didn’t find
conclusive answers, it detailed four violations, including the “abuse
and neglect” that led to the firing of five workers, along with unsafe
practices while moving him from sitting to standing and from chair to
bed.
Last week, a spokesperson for Hawthorne Place Care Centre
told the Star that its internal probe, including the work of an outside
investigator, found that Phillip’s injury was likely the result of a
staff error.
“All indications are that the injury was
unintentional — the result of an accident which occurred while the
resident was being cared for by our staff,” the emailed statement said.
“This is a highly regrettable incident, and we apologize without
reservation to the resident's family.”
Kathleen said this is the first she has heard of the home’s findings.
Hawthorne
Place is owned by Rykka Care Centres. Its managing partner, Responsive
Management Inc., said the nursing home could not go into any additional
detail because of “pending legal action” by the family. Last spring,
Kathleen, a registered nurse, hired a Toronto law firm to look into her
father’s case.
The family’s troubles began more than a year ago,
after Phillip was discharged from a Richmond Hill hospital where he had
spent two months after repeated falls, along with heart problems.
On
Oct. 25, 2017, Phillip moved into a shared room on the first floor of
Hawthorne Place, a long-term care home built in the early 1970s near
Jane St. and Finch Ave.
His
time there was expected to be short, just to get him steady on his feet
again, so he arrived with little more than his clothes and rosary
beads. If he struggled with his balance, Phillip’s mind was sharp and he
loved to read, always with a newspaper or the BBC History magazine by
his side.
Three days later, a personal support worker found
Phillip lying in bed, his sheets stained with blood, the worker told the
inspector. A deep slash in his leg cut to the bone. Staff huddled
outside his room, entering and leaving, as he lay in bed, his eyes
closed, murmuring in response to a nurse’s question: “Are you okay?” The
nurse could not hear what he said.
That afternoon, Greg Kennedy,
Phillip’s son, was driving with his mom to visit his dad when nursing
home staff called to tell him of the injury.
“When I got there, he
was in bed and his leg was bandaged,” said Greg, a supervisor at Molson
Coors, currently on disability leave. “There were five workers standing
outside his room and nobody could say what happened. He was incoherent.
He looked awful. He was grey, a kind of death look.
“I was in tears when I left there. I thought he was going to die right then and there.”
Greg
said the paramedics who rushed Phillip to Humber River Hospital told
his family to file a complaint with the ministry about the severity of
the injury and staff’s inability to describe how it happened. Kathleen
contacted the ministry, and a few days later the inspector arrived to
investigate.
The home’s administrator told the inspector that “discrepancies were found emerging from staff interviews.”
Staff
didn’t immediately report the injury to the ministry or police, as is
required when abuse is a possible cause. After the home’s administrator
learned of Phillip’s condition two days later, the ministry and police
were contacted, the report said. Kathleen and the administrator
separately reported the injury to Toronto Police, who told the Star
officers interviewed “at least two staff members” but could not confirm
how Phillip was injured. Police closed the case in January.
Hawthorne
Place fired the two personal support workers and three nurses who were
involved in Phillip’s care that day, the report said. The nurses were
reported to the College of Nurses of Ontario, the oversight body for
nurses. A college spokesperson confirmed the nurses are being
investigated.
Photographs taken by Greg show the gash was on the
outer part of Phillip’s right leg, just below the knee. It was a deep,
gaping wound.
The timeline of Phillip’s injury and how staff reacted to it are detailed in the ministry report.
At
roughly 2:30 p.m. on October 28, a personal support worker called a
registered nurse to Phillip’s room, pointing to blood on his bed sheet.
When the workerrolled up Phillip’s pant leg, the nurse
saw a “large laceration” on his outer right shin. The nurse reported
seeing “some white stuff, appeared like bone.”
This registered
nurse left Phillip without assessing him, the inspection report said,
and went to ask another nurse to measure and cover the wound. The first
nurse called the ambulance and Phillip’s family. Nobody called the
police or ministry.
The second nurse went to another part of the
home to find a measuring tape before arriving in Phillip’s room, later
telling the ministry inspector the wound was “deep with sloughs and it
was so bad (she/he) could not look at it to measure the wound.”
This second nurse left Phillip’s room without assessing him, the report said, and went to find a third nurse.
The
third nurse arrived and measured the wound at five centimetres by five
centimetres, and covered it with gauze and a bandage. Kathleen said she
believes the wound was larger.
The ministry inspectionreport
said the three nurses and two personal support workers directly
involved “denied any knowledge” of the cause of the injury, with staff
saying it likely happened between Phillip’s lunch and 2:30 p.m.
While
the inspection report doesn’t conclude what caused the injury, it notes
a personal support worker’s admission that she “transferred,” or moved,
Phillip on her own, even though his care plan had been updated a day
earlier to say he was so unsteady on his feet that he needed two people
to help him. (He weighed more than 200 pounds.)
When the inspector
later tried to re-create how Phillip had been transferred into bed, she
found that her knee pressed against the knob and a flat piece of metal
connecting the knob with the sides of the bed rail. The report said the
flat piece of metal “was not smooth.” Kathleen said the inspector told
her that this detail was considered an observation, not a conclusion of
what caused the injury.
The inspector noted that the home’s
director of care later “acknowledged the nursing team and the
physiotherapy team did not collaborate with each other” in regards to
Phillip’s assessments and the requirement he have two-worker transfers.
Phillip
Kennedy was a family law lawyer in Hamilton until retiring in 2008 when
he and his wife, Teresa, moved in with their daughter in Richmond Hill. (Steve Russell)On
the day of his injury, after Phillip returned from the dining room in a
wheelchair, the lone worker helped him out of the chair and onto the
toilet. Then the worker helped him move to his bed. The worker later
told the inspector that Phillip did not fall during those transfers. The
report said the worker acknowledged that an extra person was required.
After
the injury and Phillip’s stay in intensive care, his family requested
he be transferred back to Richmond Hill’s Mackenzie Health hospital. On
Nov. 19, three weeks after his leg wound, Phillip died. Kathleen said
the death report cited her father’s ongoing heart and kidney problems.
The
law firm, Howie, Sacks and Henry, is talking to the home through its
insurance company, Kathleen said. A lawsuit has not been filed.
“This
is a shocking injury,” said the family’s lawyer, Melissa Miller. “No
family should have to go through this. No resident of a nursing home
should have to go through this.”
Greenville, SC - South Carolina ranks at the bottom of a Wallet Hub
study when it comes to resources in place to help prevent abuse.
Many states recognize that elder abuse is a growing issue, especially in nursing homes.
State
Rep. Garry Smith (R) Greenville is working to introduce legislation
that will make it more difficult for abusers to go from one nursing home
to the next without being tracked.
"The agencies and departments
do a real good job following up on the reports, but the legislature has
done a very poor job. It's also something that we need to do to protect
those who cannot protect themselves," Rep. Smith said in a phone
interview.
Senior Action Executive Director Andrea Smith says
that nearly 5 percent of our aging population will live in a nursing
home at the end of their life.
According to WalletHub,
one in five U.S. residents will be retirement age by 2030, meaning more
aging adults will eventually need assistance and could potentially
become vulnerable to care takers.
"Giving not only support for
the seniors but for the family members that are caring for them is
another important thing that we as a community really need to get our
arms around. How do we support the folks that are taking care of
seniors," Smith says.
Andrea and her staff know that knowledge is
power, so they teach those who visit the center how to take care of
themselves, emotionally, mentally and physically.
John and Shirley Wichmann appreciate the support.
They regularly visit the Senior Action facility to see friends and get educated on issues that affect them.
"There
also are classes about things like abuse, if someone is hurting you or
if something is happening how you can report it, how you can be careful
and let people know or you can let someone here know or it can be taken
care of," Shirley said.
The NFCSP Outcome Evaluation focused on the following questions:
What
types of organizational structures and/or approaches for NFCSP services
are associated with the best participant-level outcomes?
Are
services reaching the groups targeted by the Older Americans Act (OAA),
including caregivers serving older adults with greatest social or
economic need?
To what extent do NFCSP participants also receive other home- and community-based long-term support and services?
To
what extent do NFCSP caregivers’ outcomes differ from those of
caregivers who do not receive support and services from the NFCSP?
The two-part NFCSP evaluation includes a final process evaluation report, as well as examples of assessment tools collected from State Units in Aging:
Child abuse is not simply a “family
matter” others should ignore or dismiss. We all know this.
Educational
campaigns and troubling news stories prompt people to take action when
they believe a child is being mistreated. In fact, we feel obligated to
report it to authorities.
Yet there
is less public awareness and feeling of communal responsibility when it
comes to mistreatment of older people. Elder abuse may not be on our
radar, even though older adults, particularly those who are frail or
have diminished cognitive function, can be just as vulnerable as
children.
They need to be protected too, a point
made in a recent report compiled by University of Iowa researchers for
the U.S. Department of Justice.
Researchers
focused their study on 1,000 square miles in east-central Iowa,
including Cedar Rapids and Iowa City. They held meetings, conducted
interviews, compiled information from law enforcement and reviewed laws,
regulations and other data.
They
found prosecution of elder abuse is a relatively rare occurrence. That
means abusers go unpunished, seniors continue to suffer and the rest of
us are in the dark about problems.
“One thing that
really jumped out at us was a sort of acceptance or lack of awareness
about elder abuse in general,” said Brian Kaskie, an associate professor
at the U of I and co-author of the report.
Abuse
is not necessarily physical. He’s heard stories about family members
moving into homes and taking advantage of seniors. A bank worker shared
an anecdote about an elderly customer's relative trying to withdraw
thousands of dollars. A law enforcement officer said victims themselves
frequently do not want to file charges against an abuser, particularly
if it is someone they rely on for daily help.
Kaskie hopes eventually there can be as much awareness about senior abuse as there is about child abuse and domestic abuse.
“Protecting seniors is a bipartisan issue,” he said.
Iowa
lawmakers can do more to help. They should begin by recognizing
government is not the enemy, but the best entity for helping protect the
most vulnerable people, including the more than 500,000 Iowans over the
age of 65. And government can do its job only if it’s adequately
funded.
Recommendations from the report include:
increased funding for state and county attorneys to prosecute elder
abuse; involving social workers and therapists in the investigative
process; funding for individuals and organizations who can serve as
guardians for elders; and public awareness campaigns.
Those
things are not free. Yet the GOP-controlled Iowa Legislature insists on
cutting taxes and trying to shrink the size of government. A lack of
funding for state agencies has consequences for not only older Iowans,
but all taxpayers who fund their health care through Medicare and
Medicaid.
“Victims of elder abuse have an
increased risk of hospitalization and death. Victims are also more
likely to be placed in a nursing home and are at an increased risk of
developing mental disorders such as depression and anxiety,” according
to the report.
In 2017, the Iowa Department on
Aging received about $250,000 in state appropriations specifically to
support elder abuse prevention and awareness, according to the report.
Yet budget shortfalls meant the use of those funds was limited to
supporting efforts and making referrals to understaffed government
agencies.
Iowans
understand the importance of looking out for those who cannot look out
for themselves. The people we elect to represent us need to make sure
government has the resources to do it.
This editorial is the opinion of the Des Moines Register’s editorial
board: Carol Hunter, executive editor; Kathie Obradovich, opinion
editor; Andie Dominick, editorial writer, and Richard Doak and Rox
Laird, editorial board members.
Lieutenant Teresa Miller, who heads the criminal investigations division
of the Crisp County Sheriff’s Office, reviews online information about
elder abuse and exploitation. Miller routinely investigates complaints
of elder abuse and exploitation, and says she sees a high number of
these types of cases throughout the year.
'Tis the season for scammers and crooks to take advantage
of the unaware. The victims are often the elderly, but holiday con
artists don’t discriminate by age.
People who exploit or abuse the elderly operate
all year long, and it happens a lot more often – and to a lot more
people – than one might expect, said Lt. Teresa Miller, the chief of the
Crisp County Sheriff’s Office criminal investigations division.
“In fact, we had two reports today where overseas scam
artists have called elderly people and made them believe they’re winning
a car, and all they have to do is send a Western Union money order for
$399 to pay the taxes,” Miller said. “Often in the case of at-risk
elderly, they want to believe what [scammers] are telling them.”
Elder abuse is a crime that has become more prevalent as
our population ages, and it takes many forms. It could be physical or
sexual abuse, emotional abuse, neglect, and financial exploitation.
And, especially in the case of financial exploitation, the victims often know the perpetrators.
“Financial exploitation is the most prevalent,” Miller
said. “We see family members who have control of their own parents or
grandparents’ finances and then use those funds for their own financial
gain rather than just taking care of the elderly person. That requires a
very in-depth investigation.”
Investigating financial exploitation of an elder takes
patience and expertise because it could be years before anyone learns a
crime is happening.
“In many cases financial exploitation can mean hundreds of
thousands of dollars, because it can go on for so long until someone
catches on,” Miller said. “The elderly person has no idea something bad
is happening to them.
Allan York knows this first-hand. He has a personal
relationship with at least two elderly women who have been financially
exploited, one of whom was taken advantage of by someone over the phone
and another who was scammed by someone face-to-face.
“Financial abuse is affecting these elderly citizens right
before our very eyes. There’s a lot of people suffering from it, and we
need to put a spotlight on this problem,” York said.
In the case of the woman who was victimized by someone she
knows, the financial exploitation was just the beginning of her
problems.
“We’ve seen a financial, a mental and a physical strain on
her. Her medicines were tampered with, and she almost died. That’s
nothing compared to what she lost monetarily,” York said.
Investigators take financial exploitation of the elderly
very seriously and work hard with each case to see that perpetrators are
punished, but they go into overdrive when it comes to physical abuse or
worse.
“If we find any physical abuse, they’re going to jail. It
makes the crime ‘high and aggravated’ if you abuse anyone over the age
of 65. Physical or sexual abuse of an elderly person is not going to be
tolerated,” Miller said.
You can find out more about elder abuse by going online to
aging.georgia.gov/abuse-neglect-and-exploitation-risk-adults-georgia or
contacting the state Division of Aging Services’ Adult Protective
Services at 1-866-552-4464.
At the end of an interview for a prestigious residency, I mention my physical access needs, making it clear that I can walk and manage some stairs.
“We’ve had wheelchair-bound fellows before,” my interviewer tells me.
As
soon as I hear her say “wheelchair-bound,” I feel an all-too-familiar
hollow in my stomach. It is as if I’ve been punched there. It is how I
know a description of disabled people is awry.
I
could tell her that “wheelchair-bound” is an inaccurate term, pointing
out that no wheelchair user I know is bound to a wheelchair, that every
wheelchair user I know has developed techniques and support to transfer
into a bed, or onto a toilet. But, knowing that this is an important
interview, I remain silent, which leaves my stomach feeling rather sore.
I feel this far too often. Many friends use the word “lame” to describe something, or someone, stupid. According to the Oxford Living Dictionaries,
the definition of “lame” actually means “unable to walk without
difficulty as the result of an injury or illness affecting the leg or
foot.” But, over time, “lame” has come to connote something or someone
stupid.
It is not only friends who use “lame” but also some well-known, liberal luminaries, such as Nobel Prize-winning economist and New York Times columnist Paul Krugman. In the 2012 article “An Unserious Man,”
Krugman describes Representative Paul Ryan’s response to criticisms of
his Medicare plan as “incredibly lame.” I’ve cringed when MSNBC’s Rachel
Maddow spouts “lame” from her broadcasting desk. In a 2018 Slate article, Ben Mathis-Lilley uses “lame”in his description of the political messaging of Democratic Party leaders Nancy Pelosi and Charles Schumer.
Thus,
the connection between disability and stupidity, between a physical
trait and intellectual ability, lives in our popular lexicon. Why should
this matter?
“Precision
with language is essential,” branding expert Elizabeth Talerman told me
in a recent email conversation. She continued:
We
each attach a unique meaning to what we hear. We internalize language
and interpret it based on our own experiences, from the past or the
present, from our mood in the moment. Words are first processed in the
limbic brain, our emotional center, before meaning is made through our
rationalizing frontal cortex. Kick off the wrong emotion and all
intended meaning may be lost.
The
language we use reveals assumptions that we usually don’t realize. For
example, disabled students are given “special education,” and disabled
people are seen as having “special needs.” But there is nothing special
about such education. The methods of learning might be different; there
might be a need for certain accommodations. But how could the needs of
the planet’s approximately one billion disabled people be called special?
It
wasn’t until the 1970s that millions of students in the United States,
as a matter of law, gained the right to receive the education they
deserved. The Rehabilitation Act of 1973 required schools to make accommodations for disabled students after centuries of isolating and ignoring them. In 1975, the Education for All Handicapped Children Act enforced
the right of children with disabilities to receive a free and
appropriate education. There is nothing special about a “free
appropriate education,” but many are still begrudged this legal right.
If we didn’t call this “free appropriate education” special, might such
rights be granted more easily?
How
many times have you called someone a moron? When doing so, you are
using a word coined by U.S. psychologist and eugenicist Henry Goddard.
Goddard took “moron” from the Greek root moros,
meaning dull or foolish. In true eugenic fashion, Goddard promulgated
the idea that there was a correlation between low intelligence and
criminality. To Goddard, so-called morons were a threat to the American
social fabric.
In
the first decades of the 20th century, the U.S. government oversaw the
involuntary sterilization of 60,000 developmentally disabled Americans.
In the Supreme Court’s 1927 ruling on Buck v. Bell,
Oliver Wendell Holmes asserted that these sterilizations did not
violate the due process clause of the 14th Amendment. In his decision,
the much-lauded justice wrote the infamous line “Three generations of
imbeciles are enough.” The ruling has never been expressly overturned.
When Goddard coined “moron,” the number of immigrants arriving in the United States was at record levels. JoElla Straley writes for NPR’s “Code Switch” that, “for his part, Goddard wanted to ensure there were no ‘morons’ among them.”
Writing in The New Yorker about recent media coverage of the group of migrants moving through Mexico, Masha Gessen notes:
Everyone, it seems, is calling the procession a “caravan.” The journalist Luke O’Neil has pointed out
that the word’s Persian roots conjure the image of “people trekking
across the desert with camels (ie terrorists of course).” It is less an
organized trek than it is an “exodus,” a spontaneous movement of
thousands who are fleeing a place more than they are pursuing a
destination.
Would
changing the language we use change how those deemed “other” are seen
and treated? “The choice of each word may make the difference between
piercing complacency or suffering the fate of indifference, between
creating alignment or sowing the seeds of dissent,” Talerman observed in
our conversation. “Language is the greatest tool we have for connecting
with people.”
Inaccurate
words deny that wheelchair users exist independent of their
wheelchairs, assume that those of us who are physically disabled are
stupider than non-disabled folks, begrudge the civil rights of disabled
students, endanger those who are erroneously feared (like the migrants
walking in the so-called caravan), and imply motivations that are
instead mere projection. Inaccurate words not only sow misunderstanding
but also dehumanize, which is probably why they are used — consciously
or not — in the first place.
This
is neither a matter of political correctness nor of hurt feelings.
Underlying these words are gross misunderstandings and suspect
motivations, which lead to wrongheaded policy, denial of legal rights,
and mistreatment of those with perceived differences.
It’s
no wonder that when I hear such words, my body revolts as forcefully as
if I have been punched. Seemingly innocuous words can be just as
violating as a fist. And sometimes they have just as cruel
consequences — sometimes even longer-lasting ones.
We
need to educate ourselves about the myriad words and phrases used to
undermine the accurate description of disabled lives. We need to refrain
from ablesplaining when those of us who are disabled point out these
inaccurate words. We need to interrupt the use of such words, pointing
out the inaccuracy in what is being said. We all need to think more
clearly about what we say, as well as about what the words we use
actually mean.
My
residency interviewer’s words silenced me into inaction. In that
situation, I didn’t feel empowered to interrupt and educate her about
her inaccurate words. But my non-disabled husband did write to Paul
Krugman about his use of the word “lame.” As far as we know, Krugman has
not used the word since.
Abuse happens every day and takes many forms. But vulnerable older Americans are among the easiest targets for this misconduct,
especially those who are women, have disabilities and rely on others
for care. By one estimate, elder abuse affects as many as 5 million
people per year, and more than 95 percent of all cases go unreported.
Unless states take action to prevent further abuse, the problem will
grow as America becomes an increasingly aging nation. The U.S. Census
Bureau expects the population aged 65 and older to nearly double
from 43.1 million in 2012 to 83.7 million in 2050, much to the credit
of aging Baby Boomers who began turning 65 in 2011. And by just 2030, 1 in 5 U.S. residents will be retirement age.
Fortunately, states recognize that elder abuse is a real and growing
issue. But sadly, only some are fighting hard enough to stop it.
WalletHub compared the 50 states and the District of Columbia based on
14 key indicators of elder-abuse protection in 3 overall categories. Our
data set ranges from “share of elder-abuse, gross-neglect and
exploitation complaints” to “financial elder-abuse laws.” Continue
reading below for our findings, expert commentary and a full description
of our methodology. (Click to Continue)
Deborah Ann Favorite sits in her Los Angeles apartment last month.
Favorite’s mother died after a lapse in communication about the need to
resume her thyroid medication. (Heidi de Marco/KHN)
“Oh my God, we dropped her!” Sandra Snipes said she heard the nursing
home aides yell as she fell to the floor. She landed on her right side
where her hip had recently been replaced.
She cried out in pain. A hospital clinician later discovered her hip was dislocated.
That was not the only injury Snipes, then 61, said she suffered in
2011 at Richmond Pines Healthcare Rehabilitation Center in Hamlet,
N.C. Nurses allegedly had been injecting her twice a day with a potent
blood thinner despite written instructions to stop.
“She said, ‘I just feel so tired,’” her daughter, Laura Clark, said
in an interview. “The nurses were saying she’s depressed and wasn’t
doing her exercises. I said no, something is wrong.”
Her children also discovered that Snipes’ surgical wound had become
infected and infested with insects. Just 11 days after she arrived at
the nursing home to heal from her hip surgery, she was back in the
hospital.
The fall and these other alleged lapses in care led Clark and the
family to file a lawsuit against the nursing home. Richmond Pines
declined to discuss the case beyond saying it disputed the allegations
at the time. The home agreed in 2017 to pay Snipes’ family $1.4 million
to settle their lawsuit.
While the confluence of complications in Snipes’ case was extreme,
return trips from nursing homes to hospitals are far from unusual.
With hospitals pushing patients out the door earlier, nursing homes
are deluged with increasingly frail patients. But many homes, with their
sometimes-skeletal medical staffing, often fail to handle post-hospital
complications — or create new problems by not heeding or receiving
accurate hospital and physician instructions.
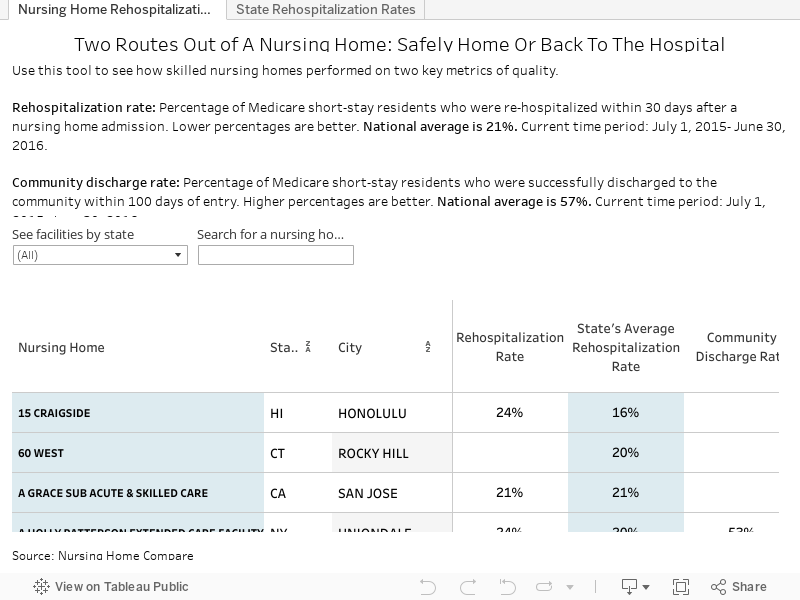
Patients, caught in the middle, may suffer. One in 5 Medicare
patients sent from the hospital to a nursing home boomerang back within
30 days, often for potentially preventable conditions such as
dehydration, infections and medication errors, federal records show.
Such rehospitalizations occur 27 percent more frequently than for the
Medicare population at large.
Nursing homes have been unintentionally rewarded by decades of
colliding government payment policies, which gave both hospitals and
nursing homes financial incentives for the transfers. That has left the
most vulnerable patients often ping-ponging between institutions,
wreaking havoc with patients’ care.
“There’s this saying in nursing homes, and it’s really unfortunate: ‘When in doubt, ship them out,’” said David Grabowski,
a professor of health care policy at Harvard Medical School. “It’s a
short-run, cost-minimizing strategy, but it ends up costing the system
and the individual a lot more.”
In recent years, the government has begun to tackle the problem. In
2013, Medicare began fining hospitals for high readmission rates in an
attempt to curtail premature discharges and to encourage hospitals to
refer patients to nursing homes with good track records.
Starting this October, the government will address the other side of
the equation, giving nursing homes bonuses or penalties based on their
Medicare rehospitalization rates. The goal is to accelerate early signs
of progress: The rate of potentially avoidable readmissions dropped to
10.8 percent in 2016 from 12.4 percent in 2011, according to Congress’
Medicare Payment Advisory Commission.
“We’re better, but not well,” Grabowski said. “There’s still a high rate of inappropriate readmissions.”
The revolving door is an unintended byproduct of long-standing
payment policies. Medicare pays hospitals a set rate to care for a
patient depending on the average time it takes to treat a patient with a
given diagnosis. That means that hospitals effectively profit by
earlier discharge and lose money by keeping patients longer, even though
an elderly patient may require a few extra days.
But nursing homes have to hospitalize patients. For one thing,
keeping patients out of hospitals requires frequent examinations and
speedy laboratory tests — all of which add costs to nursing homes.
Plus, most nursing home residents are covered by Medicaid, the
state-federal program for the poor that is usually the lowest-paying
form of insurance. If a nursing home sends a Medicaid resident to the
hospital, she usually returns with up to 100 days covered by Medicare,
which pays more. On top of all that, in some states, Medicaid pays a
“bed-hold” fee when a patient is hospitalized.
None of this is good for the patients. Nursing home residents often
return from the hospital more confused or with a new infection, said Dr.
David Gifford, a senior vice president of quality and regulatory
affairs at the American Health Care Association, a nursing home trade
group.
“And they never quite get back to normal,” he said.
‘She Looked Like A Wet Washcloth’
Communication lapses between physicians and nursing homes is one
recurring cause of rehospitalizations. Elaine Essa had been taking
thyroid medication ever since that gland was removed when she was a
teenager. Essa, 82, was living at a nursing home in Lancaster, Calif.,
in 2013 when a bout of pneumonia sent her to the hospital.
When she returned to the nursing home — now named Wellsprings
Post-Acute Care Center — her doctor omitted a crucial instruction from
her admission order: to resume the thyroid medication, according to a
lawsuit filed by her family. The nursing home telephoned Essa’s doctor
to order the medication, but he never called them back, the suit said.
Deborah
Ann Favorite holds a photograph of her mother, Elaine Essa. The nursing
home
and Essa’s primary care practice settled a lawsuit brought by the
family. (Heidi de Marco/KHN)
Without the medication, Essa’s appetite diminished, her weight
increased and her energy vanished — all indications of a thyroid
imbalance, said the family’s attorney, Ben Yeroushalmi, discussing the
lawsuit. Her doctors from Garrison Family Medical Group never visited
her, sending instead their nurse practitioner. He, like the nursing home
employees, did not grasp the cause of her decline, although her thyroid
condition was prominently noted in her medical records, the lawsuit
said.
Three months after her return from the hospital, “she looked like a
wet washcloth. She had no color in her face,” said Donna Jo Duncan, a
daughter, in a deposition. Duncan said she demanded the home’s nurses
check her mother’s blood pressure. When they did, a supervisor ran over
and said, “Call an ambulance right away,” Duncan said in the deposition.
At the hospital, a physician said tests showed “zero” thyroid hormone
levels, Deborah Ann Favorite, a daughter, recalled in an interview. She
testified in her deposition that the doctor told her, “I can’t believe
that this woman is still alive.”
Essa died the next month. The nursing home and the medical practice
settled the case for confidential amounts. Cynthia Schein, an attorney
for the home, declined to discuss the case beyond saying it was “settled
to everyone’s satisfaction.” The suit is still ongoing against one
other doctor, who did not respond to requests for comment.
Dangers In Discouraging Hospitalization
Out of the nation’s 15,630 nursing homes, one-fifth send 25 percent
or more of their patients back to the hospital, according to a Kaiser
Health News analysis of data on Medicare’s Nursing Home Compare website.
On the other end of the spectrum, the fifth of homes with the lowest
readmission rates return fewer than 17 percent of residents to the
hospital.
Get The Data
Safely Home Or Back To The Hospital?
Download the data to see how skilled nursing homes in the U.S. performed on two metrics of quality.
Many health policy experts say that spread shows how much improvement
is possible. But patient advocates fear the campaign against
hospitalizing nursing home patients may backfire, especially when
Medicare begins linking readmission rates to its payments.
“We’re always worried the bad nursing homes are going to get the
message ‘Don’t send anyone to the hospital,’” said Tony Chicotel, a
staff attorney at California Advocates for Nursing Home Reform, a
nonprofit based in San Francisco.
Richmond Pines, where Sandra Snipes stayed, has a higher-than-average
rehospitalization rate of 25 percent, according to federal records. But
the family’s lawyer, Kyle Nutt, said the lawsuit claimed the nurses
initially resisted sending Snipes back, insisting she was “just drowsy.”
After Snipes was rehospitalized, her blood thinner was discontinued,
her hip was reset, and she was discharged to a different nursing home,
according to the family’s lawsuit. But her hospital trips were not over:
When she showed signs of recurrent infection, the second home sent her
to yet another hospital, the lawsuit alleged.
Ultimately, the lawsuit claimed that doctors removed her prosthetic
hip and more than a liter of infected blood clots and tissues. Nutt said
if Richmond Pines’ nurses had “caught the over-administration of the
blood thinner right off the bat, we don’t think any of this would have
happened.”
Snipes returned home but was never able to walk again, according to
the lawsuit. Her husband, William, cared for her until she died in 2015,
her daughter, Clark, said.
“She didn’t want to go back into the nursing home,” Clark said. “She was terrified.”
There has been a three per cent increase on the number of families
waiting for a permanent place to stay with 79,880 altogether in hostels and B&Bs. This figure has risen by 56 per cent since the onset of austerity measures in 2010.
The total number of those living in B&Bs had actually fallen by
10 per cent to 5,940, but is still up a staggering 190 per cent from the
levels seen eight years ago.
Responding to the figures, Polly Neate, Shelter CEO,
said: “It’s clear that our country is in the firm grip of a housing
crisis as these figures starkly show, with older people and single
parents both bearing the brunt. If we want to protect more people from
the ravages of homelessness, the government must come up with a bold new
plan for social housing and in the short term, ensure housing benefit
covers the actual cost of rents.”
But it is not just the elderly and single-parent families that are at
risk of homelessness. The statistical release also highlighted
non-violent breakdown of a relationship with a partner, naming it the
fifth-most common reason for loss of last settled home.
“It’s good to see local authorities taking positive steps to prevent homelessness
such as finding temporary accommodation for at risk groups, but we also
need to pay closer attention to the root causes,” he said. “With non-violent relationship breakdown
being the fifth most common cause of homelessness, local authorities
should consider offering free relationship counselling to families and
individuals who may be at risk if they haven’t already done so.
The federal government announced plans Friday to crack down on
nursing homes with abnormally low weekend staffing by requiring more
surprise inspections be done on Saturdays and Sundays.
The federal Centers for Medicare & Medicaid Services said it will
identify nursing homes for which payroll records indicate low weekend
staffing or that they operate without a registered nurse. Medicare will
instruct state inspectors to focus on those potential violations during
visits.
“Since nurse staffing is directly related to the quality of care that
residents experience, CMS is very concerned about the risk to resident
health and safety that these situations may present,” the agency said in
a notification to state inspection offices.
The directive comes after a Kaiser Health News analysis found there are 11 percent fewer nurses providing direct care on weekends on average, and 8 percent fewer aides.
Residents and their families frequently complain the residents have
trouble getting basic help — such as assistance going to the bathroom —
on weekends. One nursing home resident in upstate New York compared his
facility to a weekend “ghost town” because of the paucity of workers.
Richard Mollot, executive director of the Long Term Care Community
Coalition, an advocacy group in Manhattan, welcomed the new edict but
said it was only necessary because state inspectors have not been
properly enforcing the rules already on the books.
“The basic problem is the states don’t take this seriously,” Mollot
said. “How many studies do we have to have, year after year, decade
after decade, saying it all comes down to staffing, and there are very
few citations for inadequate staffing and virtually all of them are
identified as not causing any resident harm?”
CMS said it will identify potential violators by analyzing payroll
records that nursing homes are now required to submit. Those records,
which became public this year, showed lower staffing than what
facilities had previously told inspectors during their visits, according
to the KHN analysis.
“CMS takes very seriously our responsibility to protect the safety
and quality of care for our beneficiaries,” CMS Administrator Seema
Verma said in a statement.
The nursing home industry criticized the heightened scrutiny.
“Unfortunately, today’s action by CMS will enforce policies that
makes it even more difficult to meet regulatory requirements and hire
staff,” said Dr. David Gifford, senior vice president of quality and
regulatory affairs at the American Health Care Association, an industry
trade group, in a written statement. “Rather than taking proactive steps
to address the national workforce shortage long-term care facilities
are facing, CMS seems to be focusing on a punitive approach that will
penalize providers and make it harder to hire staff to meet the shared
goal of increasing staffing.”
Currently, a tenth of inspections must occur during “off hours,”
which can be either a weekend, or during a weekday before 8 a.m. or
after 6 p.m. But for facilities that Medicare identifies as having lower
weekend staffing, half of those off-hour inspections—or 5 percent of
the total — must be performed on Saturdays or Sundays.
Medicare requires nursing homes to have a registered nurse on site
for at least eight hours every day, but according to the payroll
records, a quarter of nursing homes reported no registered nurses
available at least one day during a three-month period. Since July,
Medicare’s Nursing Home Compare website for consumers has highlighted homes that lack sufficient registered nurses and lowered their star ratings. Nursing Home Compare has downgraded ratings for 1,402 of 15,600 facilities for gaps in registered nurse staffing, records show.
The new directive instructs inspectors to more thoroughly evaluate
staffing at facilities Medicare flags. The edict does not mean a flurry
of sudden inspections. Instead, Medicare wants heightened focus on those
nursing homes when inspectors come for their standard reviews, which
take place roughly once a year for most facilities.
But what may appear to be staffing scarcities in payroll records may
instead be clerical problems in which nurse hours are not properly
recorded, say some nursing home officials.
Katie Smith Sloan, president of LeadingAge, an association of
nonprofit providers of aging services, said in a statement that some
homes are still struggling to adapt to the new data collection rules.
“We’ve been voicing our concerns to CMS and will continue to do so,” she said.
A 67-year-old woman who has trouble walking was reportedly left in a wheelchair overnight after her flight from Chicago to Detroit was cancelled on Friday.
Olimpia Warsaw’s son Claude Coltea told CBS Chicago
that she had flown to Chicago to attend her ex-husband’s funeral. On
the way there, her luggage was lost. On the way back, she was abandoned
in the airport.
Her
son reportedly dropped her off at her gate, checked that her flight was
on time, and then headed to catch his own flight. But when her flight
ended up getting cancelled, no one helped her get to a hotel, according
to her son.
“All
we wanted was someone to pause and say, ‘You know what, can we just
make sure this human being is safe and then we can all go home,’” Coltea
told CBS. “Not one person did that.”
After
a porter was assigned to help Warsaw, Coltea claims they took his mom
to the front of Chicago O’Hare International Airport and then left
because their shift was over. Coltea said Warsaw has trouble
communicating and wasn’t able to find a way to the hotel on her own.
“She
actually had to find a random passenger to help her out just to go to
the bathroom because the porters had already left for the night,” Coltea
told CBS.
American Airlines
said in a statement to Yahoo Lifestyle that its team “is deeply
concerned about what occurred Friday evening” at O’Hare. “This is not
the level of service we aspire to provide to our customers, and we
apologize to Ms. Warsaw and her family for letting them down.”
The
airline added that it has launched an investigation with its Chicago
team, and is working with the vendor it utilizes to provide wheelchair
services at O’Hare to “ensure this does not happen again.” American Airlines said its staff has spoken with the family multiple times and refunded Warsaw’s ticket.




/https://www.thestar.com/content/dam/thestar/news/investigations/2018/12/03/an-81-year-old-grandfather-his-gruesome-leg-wound-and-no-explanation-from-caregivers-the-story-of-phillip-kennedys-three-days-in-a-toronto-nursing-home/family_photo.jpg)
/https://www.thestar.com/content/dam/thestar/news/investigations/2018/12/03/an-81-year-old-grandfather-his-gruesome-leg-wound-and-no-explanation-from-caregivers-the-story-of-phillip-kennedys-three-days-in-a-toronto-nursing-home/kennedy_headshot.jpg)